It’s been a couple of months since I published an article that was written my husband, on tips to stay safe during the viral pandemic that hit our planet. In our day jobs we study the biochemistry of infectious diseases. A lot of what was written then can be updated to reflect new findings, new research, as physicians and scientists learn more about the virus and its transmission. I am publishing today his update on the previous post. I would also like to share a very good article that debunks a damaging video (Plandemics) that unfortunately has gone viral.
Without further ado, here is Dr. Phillip Klebba….
Let’s reassess. On March 16, 2020 I advised on how to avoid COVID-19. In the ensuing eight weeks 73 US deaths exploded to 81,000; 6500 deaths in China became 285,000 deaths worldwide. More than a quarter million people already perished, but we are not free of COVID-19 yet. Nevertheless, in many countries, including the US, officials are underestimating and/or misrepresenting the severity of this pandemic. All 50 states plan to relax virus containment measures, in essence relegating health behind the economy. The federal government is not promoting policies that protect us from the virus. In that sense, we are mostly on our own to protect ourselves. Make no mistake, COVID-19 is all around us, much more widely distributed than 2 months ago, and it hasn’t lost any of its lethality. Fortunately, we’ve learned a lot about COVID-19, which I summarize below along with a list of protections, that is modified from these insights. Besides the precautions I previously recommended, some additional actions are needed as COVID-19 spreads and multiplies in places near you. From lessons learned during other viral pandemics (Spanish Flu, Polio, Asian Flu, Hong Kong Flu, Ebola), and what is now known about COVID-19, I updated the advisories on how to protect yourself from infection. The most important realization is that the virus appears transmissible through the air. What follows is a summary of what’s known about COVID-19.
A. It’s highly contagious. The R0 of COVID-19 was initially estimated as 2.2 – 2.7, but other projections put it higher (R0= 5.7; Sanche et al., 2020). In other words, on average a single person may infect 5-6 other people.
B. It’s deadly. As of May 11, its mortality rate worldwide is 6.9%; in the US it is 5.96%. In other words, approximately 6% of people who contracted it are dead. The 2019 seasonal flu had mortality of 0.1%; the 1918 Spanish flu had mortality of 2.5%.
C. It’s unusually hardy. It survives for a day on cardboard and several days on surfaces like plastic and stainless steel. It is less durable in the air (3-4 h) or in sunlight (at 85oF, only a few minutes).
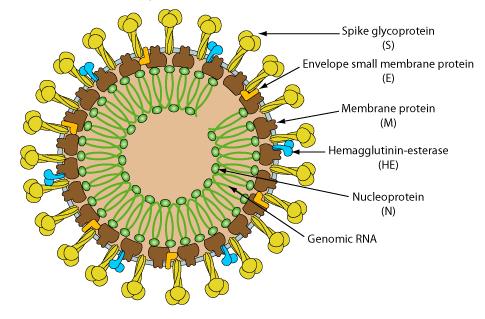
D. Transmission on surfaces and through the air. The most significant news is that COVID-19 is transmissible through the air. Its diameter of 100 nanometers (nm) is similar to or slightly smaller than that of other airborne viruses, like measles (100-300 nm), chickenpox (150-200 nm), influenza (80-120 nm), norovirus (23-40 nm), adenovirus (90-100 nm). Although viruses are most commonly transmitted on contaminated surfaces (fomites), several scientific reports also show airborne transmission of COVID-19.
- Contaminated surfaces. A study of Huoshenshan Hospital in Wuhan, that was filled with COVID-19 patients, took swabs of surfaces in the intensive care unit (ICU) and general ward (GW) (Guo et al., 2020). They tested for viral RNA, including on hand rails, bed posts, sinks, toilets, cell phones, computer keyboards, mice, screens, and floors. All ICU surfaces were heavily contaminated (~75% positive); GW surfaces less so (~25% positive). Notably, every swab from the floor of the adjacent pharmacy, that did not house any patients, was contaminated, indicating that nurses and physicians were tracking COVID-19 from the ICU/GW to the pharmacy on their shoes. Air samples from the ICU also contained viral particles (~35% positive)
- Respiratory droplets from coughing and sneezing. Transmission by virus floating in the air is a complicated combination of the density of airborne viral particles, the length of time someone breathes them in, and the infectious dose of the virus. For a detailed discussion see this link. Airborne transmission does occur, especially during protracted exposure to aerosolized virus in closed spaces. Another study measured COVID-19 RNA in the air of Renmin and Fancang hospitals in Wuhan (Liu et al., 2020). Well ventilated areas had little evidence of the virus, but the air in poorly ventilated, small spaces (e.g., mobile toilets) was heavily contaminated. A third study of virus shedding by patients at the University of Nebraska Medical Center (Santarpia et al., 2020) confirmed that COVID-19 was shed during respiration, toilet, and as fomites, indicating that infection may occur by both direct and indirect contact, including by airborne transmission.
E. Trajectory of the COVID-19 pandemic. To see the data I use this site. The situation is shocking: after 3 months, 4.2M people were infected worldwide, resulting 280K deaths; 1.37M people were infected in the US, resulting in 81K deaths. Graphs of these trends show both infections and mortality leveling off, but still increasing.
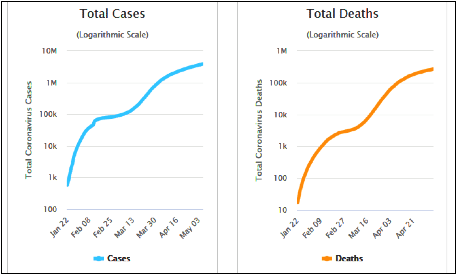
Worldwide (Fig. 1), the Jan – Mar data came from China; later data show COVID-19 spreading around the world where it is still not controlled.
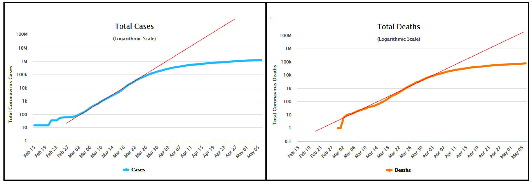
In the US (Fig. 2) the deviation of blue and orange lines from the red lines shows the positive impact of social distancing. Yet, at present (i.e., the past few weeks) we are still adding >25K new infections and >2000 deaths per day. Without a vaccine or anti-viral drug, if we abandon social distancing the virus will resume its spread to new places and people. The slope of both curves will rise again, as occurred worldwide when COVID-19 moved from China to other nations. The upshot is that, relative to March 1, 2020 (75 cases), COVID-19 has infected thousands of new venues across the US (1.3M cases), and is poised to return to rapid growth in our population. It’s a threatening situation, especially for people in a risk group: the elderly, immunosuppressed, diabetic, cardiovascular, cancer patients.
SUMMARY OF PROTECTIVE PROCEDURES
(Added to the previously suggested practices, not replacing them)
- Shoes. Select an old pair of shoes to wear on shopping trips or other excursions. Keep them in the garage, change into them when you depart the house, take them off when you return home, and then disinfect the soles with 10% bleach when you remove them.
- Face covering. Cover your nose and mouth in public. Masks and scarves are uncomfortable and embarrassing; get over it. Once you put it on, do not touch it until you return home. Sterilize your hands with 70% alcohol or 10% bleach before removing your mask. Covering your face reduces your risk of infection, the risk of unknowingly passing COVID-19 to someone else, and shows solidarity with federal CDC guidelines, which is good for everyone. If businesses are to open, then we need to do it as safely as possible, and that means with face coverings.
- Hands. Keep your hands below your shoulders; regularly sanitize them; never touch your face.
- Social distance. Stay 6-feet away from everyone you encounter. This takes thought and practice, because we have a habit of standing close to people we talk to. Keep your distance and do not engage in long conversations with anyone.
- The outside world. Consider everything outside of your home contaminated and contagious; protect your home by disinfecting everything that enters it. Go out as infrequently as possible, and when you go carry disinfectants with you, to sanitize your steering wheel, your shopping carts and your hands after touching anything questionable.
- Home-sweet-home. When you return home, carefully and meticulously disinfect your hands with alcohol or bleach, and then thoroughly wash them with warm soap and water. Change your clothes. Frequently wash your hands, especially before eating.
Scientific References:
- van Doremalenet al. 2020. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1.N. Engl. J. Med. 382: 16
- Sanche et al., 2020. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerging Infectious Diseases 26 (7): July 2020.
- Guo et al., 2020. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China. Emerging Infectious Diseases 26 (7): July 2020
- Liu et al. 2020. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Naturehttps://doi.org/10.1038/s41586-020-2271-3
- Santarpia et al. 2020. Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center. medRxiv doi: https://doi.org/10.1101/2020.03.23.20039446